Welcome to Isaree: Building the Agentic Future of Healthcare
I still remember a conversation I had with a physician friend late one evening. She told me how she was struggling to integrate AI tools into her clinical workflow, each one promising to help, but none fitting naturally into how she actually practiced medicine. Every new model meant another login, another dashboard, another step away from her patients.
A few months later, while doing strategic consulting work for a large private hospital group, their CIO shared a similar frustration, but from the other side. Clinicians in his network wanted to experiment with over 300 different AI solutions. “It’s starting to feel like the 1990s all over again,” he said, “when every department bought its own software, and we ended up with hospitals running two thousand disconnected applications. Completely unmanageable.”
Those two conversations, one from the front lines of care, one from the heart of hospital IT, captured the same tension from opposite ends. Clinicians want freedom and innovation. Administrators need safety and stability. But the architecture of current AI systems can’t deliver both.
That’s when the idea for Isaree took shape.
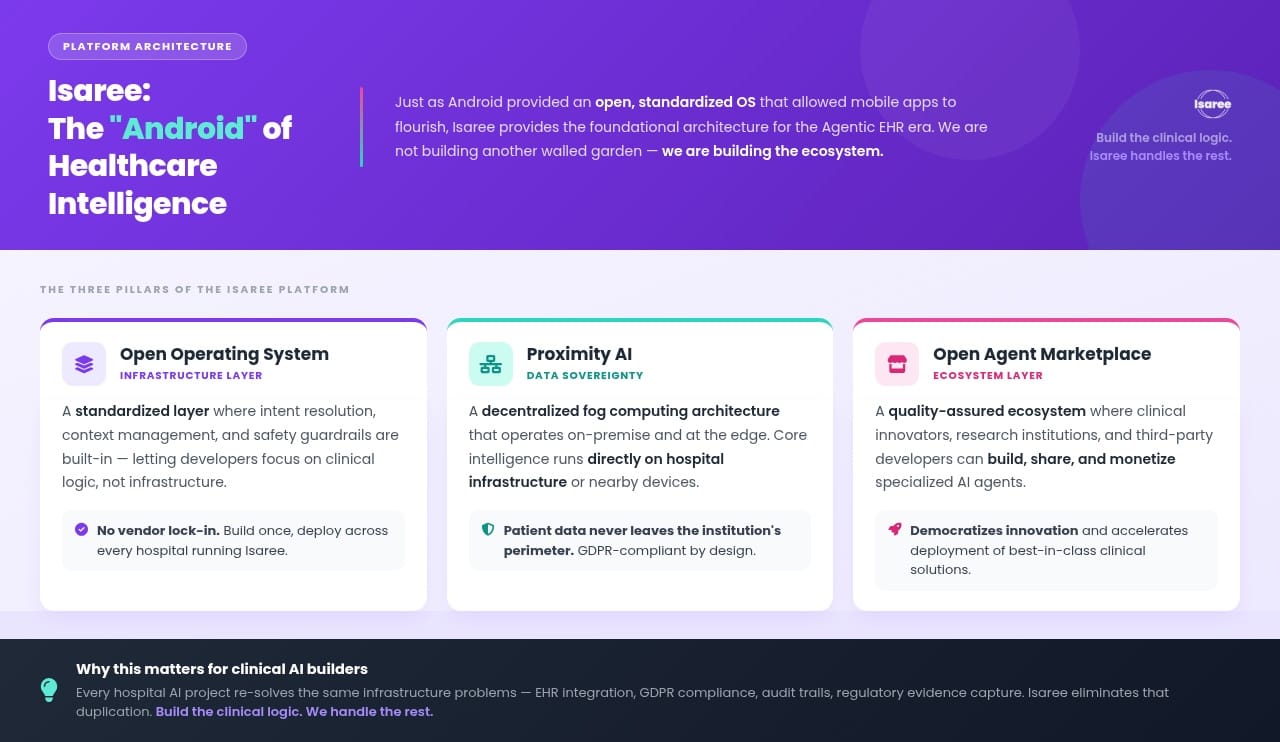
Isaree means freedom in Thai. For us, it represents the freedom to design AI that actually works for clinicians — seamlessly, securely, and sustainably. We’re not building another cloud-based charting tool or a monolithic AI that tries to solve healthcare from a distant server farm. We’re building an operating system for clinical AI that brings intelligence directly to the point of care.
The Last Mile Problem in Clinical AI
The healthcare industry has mastered the AI pilot. But scaling those pilots into clinical reality is a different story. We are spending billions of dollars to publish papers that never reach patients. By the end of 2024, there were close to 100,000 medical AI publications on PubMed alone. Yet, when a recent Stanford-Harvard review examined hundreds of influential clinical AI studies, they found that only 5 percent actually tested models using real clinical data.
Across industries, organizations capture only 20 to 25 percent of AI's potential value. In healthcare, the translation failure rate is staggering, up to 80 percent of healthcare AI projects fail to scale beyond the pilot phase. This gap between building a predictive model and actually integrating it into a clinical workflow, the "last mile", is where most innovation goes to die.
Why? Because most AI tools are built by engineers, not clinicians. They are designed for cloud infrastructure, introducing latency, connectivity dependencies, and massive compliance risks under frameworks like the EU AI Act. They force clinicians to adapt to the software, rather than the software adapting to the clinician. The result is "activated shelfware", tools that are technically live but rarely used because they lack a clear, immediate benefit to the person delivering care.
This is not a technical limitation we are working around. It is an architectural flaw in how medical AI is currently deployed.
Proximity AI and Hybrid Inference
Isaree takes a fundamentally different approach. We are implementing what we call Proximity AI. This means we bring the agents as close as possible to the space and time of demand.
Robert C. Wolcott and Kaihan Krippendorff describe Proximity as the defining force of our era: digital technologies pushing the production and provision of value ever closer to the moment of actual demand. Just-in-time anything, anywhere, anytime.
We apply this principle directly to clinical AI.
We call it Proximity AI. We bring the agents as close as possible to the space and time of demand.
Whenever possible, the intelligence lives entirely on the device in your hand. No data leaves your control. When a GP in a rural clinic needs to draft a referral letter, she does not need a stable Wi-Fi connection or a cloud round-trip. She uses an on-device agent that understands her patient's longitudinal record instantly, securely, and offline.
However, we understand the reality of hospital IT infrastructure. Not every employee has access to a high-end mobile device capable of running a 10B parameter model locally. That is why Isaree supports hybrid inference. We seamlessly integrate external agents and on-premise models via secure protocols. If the device cannot handle the compute, the inference shifts to the nearest secure node, be it an on-premise hospital server or a trusted external agent, without breaking the clinical workflow or compromising the patient's longitudinal context.
This architectural flexibility changes the power dynamic in healthcare. The clinician, not a cloud server, not a vendor, holds the intelligence, regardless of the hardware in their pocket.
Furthermore, Proximity AI forces the entire ecosystem to push for efficiency. By orchestrating small, specialized agents based on sparse language models, we drastically reduce computational waste. Recent research demonstrates that shifting from massive monolithic models to orchestrated, task-specific small models can slash energy consumption by up to 90%, and in some implementations, reduce energy use by a factor of 100 to 300 compared to standard approaches. Isaree is not just building a more capable AI; we are building a radically more sustainable one.
The Clinician-Built Ecosystem
But the true power of Isaree lies in who builds the tools. We believe that the physicians of the future must be both users and creators of AI.
Centralized, highly generalized models are difficult to certify for specific, regulated domains like healthcare. Specialized, open-source models, however, can be rigorously tested and certified. That is why we are launching the Isaree Community Hub, an open ecosystem where clinicians and scientists can build, verify, and share specialized AI agents.
Think of it as the App Store for medical AI. A cardiologist in Berlin can build an agent for pre-consultation screening. A pediatrician in Barcelona can download it, adapt it for her practice, and share her version back. Clinicians or researchers own the agents they build. They control them, share them, and eventually, they can commercialize them.
This agentic orchestration allows hundreds of small, specialized models to collaborate and collectively outperform monolithic systems. It creates compounding network effects: each new agent makes the platform more valuable for every clinician on it.
Our Mission
Together with my co-founder Mandana Ahmadi, we founded Isaree in Berlin because we believe in the power of decentralized, sustainable, and privacy-protecting technology. The transition to an agent ecosystem, a network of millions of specialized AI agents, is a new layer of value creation that will free healthcare professionals from bureaucratic burdens
We are building the infrastructure for that future. We are solving the last mile by putting the tools of creation directly into the hands of the people delivering care.
The future of healthcare AI is not locked in a distant data center. It is arriving at the exact space and time of demand. And the clinicians building alongside us are proving it works.
I hope you feel the same and are inspired to join our mission to build the future of medical AI together,
Bart
CEO Isaree
PS: Some of you are receiving this because you subscribed to my innovation newsletter, where I share insights and reflections on digital health and emerging technologies. If you’d prefer not to receive future updates, you can easily unsubscribe using the link below.