60,000 Reasons the Hospital AI Era Belongs to Clinicians, Not Cloud Vendors
Three weeks ago, I wrote about why cloud APIs are already obsolete in healthcare. Last week, I wrote about the bottleneck shifting, how the new interface for building software is natural language, and how clinicians, not engineers, are becoming the new builders.
Then Prosus dropped a report that validated both arguments with 60,000 data points.
Prosus, the €100B+ company behind Just Eat Takeaway, iFood, and PayU - gave 40,000 employees a platform to build their own AI agents. In 18 months, those employees built 60,000 agents. No central mandate. No engineering degree required. Just people solving their own problems with the right tools.
The numbers inside the report are remarkable. Let me give you the ones that matter for healthcare.
The power law that will reshape hospitals
Prosus found that 2% of AI agents drive disproportionate business impact. The rest serve narrower, individual workflows. This isn't a bug, it's the distribution.
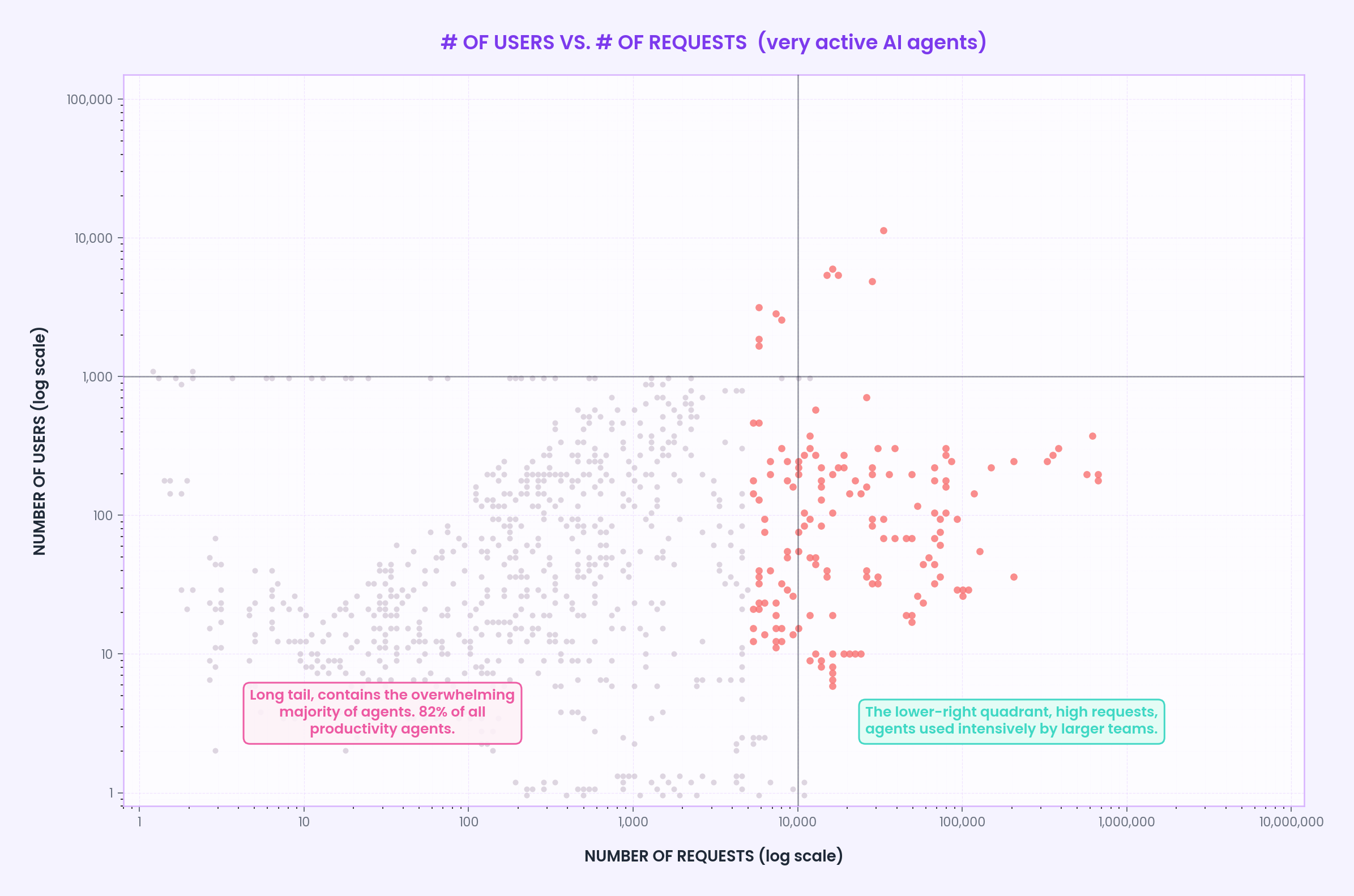
The lower-left quadrant, low users, low requests, is where the long tail lives. 82% of all productivity agents sit here. These are the agents you use a few times a day, maybe a few times a week. The clinical guideline lookup you fire once per shift. The "summarise this patient's history for me" prompt. The inbox triage bot that sorts your messages but doesn't do the work for you. Each one saves under 20 hours per month individually, NHS England's Copilot trial found an average of 43 minutes saved per staff member per day, roughly 14 hours a month. That sounds modest until you do the maths: multiply that across 500 clinicians and you're reclaiming 7,000 hours a month. At a 1,000-bed hospital, that's an entire clinical department's worth of capacity. The lower-left quadrant isn't unimpressive, it's a quietly enormous, distributed form of productivity that compounds across every person in the building.
The lower-right quadrant, high requests, low users, is where the documentation time killers live. These are agents hit relentlessly by the people who depend on them. The ambient scribe that fires on every single patient encounter, 20 to 30 times a day per clinician, saving 16 minutes of documentation time per session, that's the JAMA multisite study across 8,581 clinicians. The prior auth agent that a revenue cycle team of 12 slams 50,000 times a month, collapsing a 9-minute human review into 38 seconds and saving an 18-hospital network $6.2 million in year one. The pathology department's lab triage agent that runs on every result. These agents represent a slice of the 17% middle tier, saving 20 to 173 hours per month, up to a full FTE. They're not used by everyone. They're used constantly by the people who need them most.
And then there's the top of the chart, the smattering of outliers with thousands of users and hundreds of thousands of requests. Less than 1% of agents, delivering thousands of hours of work per month. In Prosus's case, one of them unlocked an $83M revenue stream. In healthcare: the agents that orchestrate entire care pathways across primary and secondary care, that manage chronic disease cohorts autonomously. The agents nobody's built yet, because nobody's given clinicians the tools.
The number that should terrify every hospital CIO
Prosus found that most AI models are now "good enough." Since Claude Sonnet 4, they've observed diminishing returns on every new model. Users stop caring about model choice entirely once their agent works.
This is devastating for the cloud API business model in healthcare.
We modeled the 3-year total cost of ownership for a 10-clinician practice running 5 AI agents per day. Local AI on Apple Silicon: €9,315. Claude 4 Sonnet via cloud API: €75,673. A credit-based orchestration platform like Manus: €183,298.
The models are good enough. The cloud costs aren't.
And in healthcare, cost isn't just financial. It's regulatory. The EU AI Act makes certifying a cloud API, with silent model updates, cross-jurisdiction data processing, and no audit trail, structurally nearly impossible.
A frozen, auditable SLM running on a clinician's own device? That's certifiable, and that's why we are building Isaree.
The 14% that hospital IT departments will ignore at their peril
Prosus categorized every single one of the 60,000 AI agents by which department they belonged to. The largest share, 18%, sat in Data Analytics & Market Intelligence. Next came Operations at 15%.
The third largest wasn't a department at all. 14% of all agents sat outside any formal department. These were personal AI assistants, built by individual employees, for themselves. Not commissioned by IT. Not approved by management. Just people solving their own problems with the right tools.
Bigger than Marketing. Bigger than Finance. Personal AI.
Now translate that to a hospital. A few weeks ago, we spoke to a friend who runs a hospital in Switzerland. I asked him if the concept of personalised AI agents, agents built by clinicians, for clinicians, was valuable to him. His answer was immediate: he said the potential isn't in the big departmental deployments. It's in what happens when every clinician has an agent that knows their workflow, their patients, their preferences. The personal stuff. The 14%.
He's right. And the same thing is already happening, with or without IT approval. Clinicians are building their own agents. Inbox triage. Guideline lookups. The "what did we do last time for a patient like this" prompt. They'll run on phones, on laptops, on whatever hardware is available.
The only question is whether they'll run on the clinician's device, or on a cloud API that charges by the word, changes its pricing overnight, and ships patient data to servers in jurisdictions the clinician has never heard of.
The fork in the road
Prosus's end-state vision is autonomous AI-led organizations, departments run by AI with minimal human oversight. That's the logical endpoint of a centralized cloud platform: if the platform orchestrates everything, why not let it run everything?
Healthcare can't go there. Not ethically. Not regulatorily. Not clinically.
The alternative is what we're building at Isaree: an on-device AI agent platform where clinicians build, own, and potentially commercialize their own agents. Running on Apple Silicon. 100% offline capable. Patient data never leaves the device, without the users consent.
The Prosus report proves the model works, 60,000 agents in 18 months, built by non-technical employees solving their own problems.
Now imagine what 60,000 clinicians could build.
We're starting with 50, across 14 countries. Targeting 1,000 at the Berlin Healthcare Hackathon this year. Feel free to join!
But here's what I really want to say to hospital leaders reading this:
The Prosus model is repeatable. You don't need 40,000 employees to start. You need a platform that lets your staff build agent flows, and deploy them immediately, on-device, solving real problems the same day they're built.
Imagine what happens when you teach a department of clinicians how to build their own AI agents. The cardiologist who automates her discharge summaries. The nursing team that builds a shift handover agent. The revenue cycle staff who turn a 9-minute prior auth into 38 seconds. Now multiply that across your entire organization.
That's what Isaree offers: not pre-built agents delivered by a vendor, but the tools and training for your staff to build their own, running locally, keeping patient data on-device, at a fixed cost that doesn't punish you for using AI more.
If you want to repeat the Prosus model inside your hospital, teach your staff to build, deploy, and own their agents, let's talk. We offer the most advanced end-end platform and agent harness at the lowest costs.
The bottleneck has shifted. The tools are ready. The question isn't whether clinical AI agents will be built, it's who will build them, and on whose infrastructure.
I keep getting asked the same question: will clinicians actually build their own AI agents?
It reminds me of the question nobody remembers asking in the 1980s: will people actually run a word processor on a personal computer? Back then, word processing meant WordPerfect on MS-DOS, arcane key combinations, command-line interfaces, something you needed training to operate. The idea that every office worker, every student, every person would one day just… type into a screen and print, was absurd. Until the interface changed. Until it became more natural.
Natural language is the new GUI. The clinicians who couldn't write a SQL query or configure a cloud API are the same people who can describe exactly what they need in plain English, or Dutch, or Arabic, or any language. That's the interface now.
The only question is whether the agents they build will run on their terms, on their devices, with their data staying local.
We believe the answer is yes, and we would love to work with you to prove it,
Bart
P.S. — We're onboarding our second cohort of clinical innovators. If you want to build the agents your hospital needs, on your own terms, join the waiting list.